17 y/o male with muscle weakness
Case Authors: Steve Wood, PhD
Tracey Milligan, MD
Case Based Learning
You will work on this case in 8 groups of 7 students per group. The group should discuss all the questions (10 min) and then each member of the group should pick one of the 7 questions to research during the during the next 30 minutes of the first session and submit their answer using this form. During the last 10 minutes of the first session, the 7 students who researched each question will form a new group (e.g., 7 students who worked on question 1) and take 10 minutes to discuss their individual answers and make plans for coming up with a group consensus answer to be presented during the second session for the case. During the second session, one or more students from each group will present the answer to their group’s question for 5 minutes followed by 2 minutes for questions from the class.
Learning Objectives
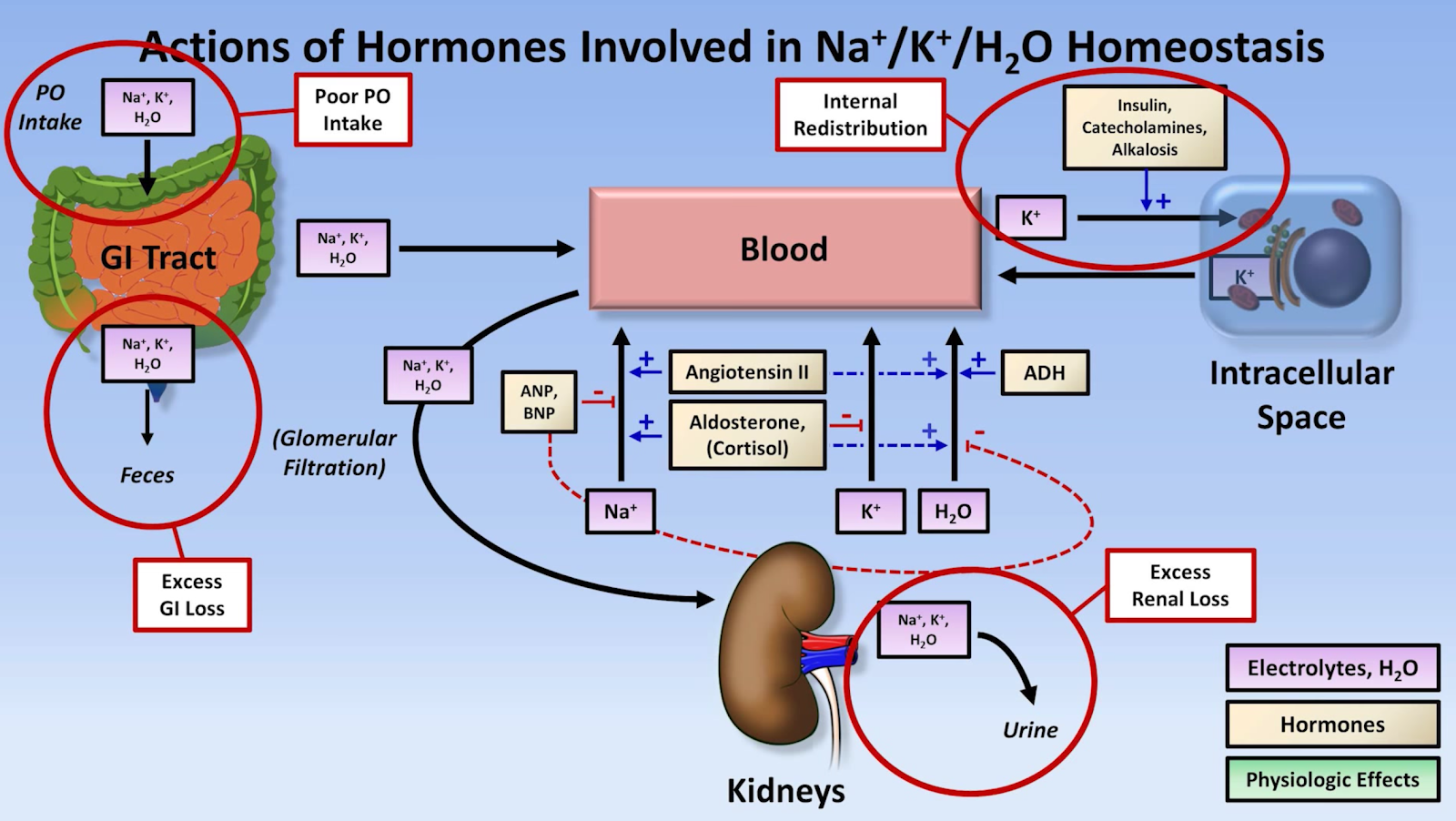
Draw a concept map and explain the mechanisms (hormonal, renal, cellular) involved in potassium homeostasis.
Draw and label the phases of an action potential for a skeletal muscle cell, cardiac muscle cell, and sinoatrial node.
Describe the effects of hypokalemia and hyperkalemia on the resting membrane potential and potassium conductance of cells including nerve and muscle.
Describe how surreptitious use of diuretics can cause hypokalemia and explain how one diuretic (acetazolamine) can be used to treat hypokalemia.
Explain the mechanisms of muscle weakness in hypokalemia.
Describe the genetics and molecular mechanisms of hypokalemic periodic paralysis.
Explain the mechanisms that lead to transcellular shifts of potassium. Describe how marijuana intoxication may lead to hypokalemia.
Bonus question (anybody can do this one): Explain the abnormal findings on the EKG.
Pre-study
Costanzo - sections on membrane potential, Nernst equation, etc.
Gordon Hu is a 17-year-old member of his high school wrestling team. He is 5’ 10” tall and competes in the 145 - 150 lb. division. He struggles to make this weight for matches as his weight is normally 160 lbs. He is extremely muscular and exercises frequently outside of practice including cardio and strength training. He doesn’t drink or smoke cigarettes but does smoke marijuana with his friends.
He knew it was normal to be tired and feel weak after a hard practice or match, but lately he had noticed extreme weakness and his legs felt “like rubber”. He thought that maybe he had low blood sugar so he made it a point to do some “carb loading” before a match. Instead of improving his symptoms, this seemed to make them worse. After his most recent match, he had to carried off the mat after he was pinned, suffering his 3rd straight loss. After he collapsed, Gordon was terrified when he discovered that although he was conscious, he couldn’t open his eyes or speak for about 30 seconds; then he was o.k. but still had to be helped off the mat.
Gordon’s parents were at the wrestling match and were very alarmed at what had happened. His father remembered having similar problems when he was a high school athlete. They told Gordon they were going to make an appointment with the family doctor. The next morning, they met with Dr. Rhodes, their family physician. Dr. Rhodes talked to Gordon about his problem and made the following notes on Gordon’s chart:
Gordon’s symptoms were recent onset. He did not have any problems like this when he was a child. He started noticing some weakness after he went out for wrestling in 10th grade (2 years ago). The problem only occurred once in awhile. Sometimes he would have no problems for 6 months, and then experience weakness several times a month. Gordon has no siblings. He reports having several girlfriends and is sexually active. No recent travel. Childhood illnesses were chickenpox, mumps, and measles. Physical exams have been normal. Denies cigarette and alcohol use. He smokes marijuana “occasionally”. Due to physique, inquiry was made re: steroid use. Pt. denies using any steroids. Gordon’s father reported similar problems when he was involved in high school athletics. He remembered that some “supplement” prescribed by the family doctor made it better.
Dr. Rhodes took a blood sample and sent it to the lab next door for a CBC and electrolyte panel. He also took a muscle biopsy for testing. While waiting for the results he did a physical exam:
Physical Exam
General - healthy young man, alert, oriented.
Vital signs
Oxygen saturation 98%
Blood pressure 120/80 mm Hg
Pulse 66 beats per minute
Respiration 12 bpm
Weight 160 lbs
Height 5 ft. 10 in
Temperature 98.6 F
Laboratory Tests/Investigations
CBC
Hb 15 g/dL (normal 14-18 g/dL)
Hct 45 % (normal 42-52%)
White blood count (WBC) 12 x 103 (normal 5-10 x 103/mm3)
Neutrophils – elevated
Lymphocytes – nl
Monocytes - nl
Eosinophils – nl
Basophils - nl
Platelets 450,000 (normal 150,000 – 400,000/mm3)
Electrolytes
Na+ - 135 (normal 135 – 145 mEq/L)
K+ - 4.4 (normal 3.5 – 5 mEq/L)
Cl- - 110 (normal 100 – 110 mEq/L)
Because the test results were mostly normal, Dr. Rhodes decided to repeat the blood test after Gordon had done 40 pushups in the office. The electrolyte results were:
Electrolytes
Na+ 135 (normal 135 – 145 mEq/L)
K+ 2.2 (normal 3.5 – 5 mEq/L)
Cl- 110 (normal 100 – 110 mEq/L)
A 12 lead EKG was obtained because of the low K+
Normal EKG
Dr. Rhodes told Gordon that he has a condition called hypokalemic periodic paralysis. He explained that there is no cure but it can be treated. He explained that it is an inherited trait due to a gene mutation.
Discuss the following questions/learning issues and each member pick 1 of them for presentation during the second session. Submit your answers using this form.
Draw a concept map and explain the mechanisms (hormonal, renal, cellular) involved in potassium homeostasis.
Also, to amplify the renin-angiotensin-aldosterone system:

High potassium is one of the signals that stimulates production of renin which catalyzes the conversion of angiotensinogen to angiotensin I to start the signalling pathway.
2. Draw and label the phases of an action potential for a neuron, skeletal muscle cell, cardiac muscle cell, and sinoatrial node. 
3. Describe the effects of hypokalemia and hyperkalemia on the resting membrane potential and potassium conductance of cells including nerve and muscle.
Hyperkalemia effects on cardiac muscle action potentials are summarized in this figure: During phase 4, the resting membrane potential is depolarized (less negative) according to the Nernst equation

Phase 0 of the action potential occurs when voltage gated
sodium channels open and sodium enters the
myocyte down its electrochemical gradient.
The rate of rise of phase 0 of the action potential (Vmax)
is directly proportional to the value of the resting
membrane potential at the onset of phase 0. This is
because the membrane potential at the onset of depolarization
determines the number of sodium channels
activated during depolarization, which in turn determines
the magnitude of the inward sodium current
and the Vmax of the action potential.
Hyperkalemia also has profound effects upon phase
2 and phase 3 of the action potential. After the rapid
influx of sodium across the cell membrane in phase 0,
potassium ions leave the cell along its electrochemical
gradient, which is reflected in phase 1 of the action
potential. As the membrane potential reaches –40 to
–45 mV during phase 0, calcium channels are stimulated,
allowing calcium to enter the myocyte. The maximum conductance of these channels occurs approximately 50 msec after the initiation of phase 0 and is reflected in phase 2 of the action potential.
During phase 2, potassium efflux and calcium influx offset one another so that the electrical charge across the cell membrane remains the same, and the so-called plateau phase of the action potential is created (Fig. 3). During phase 3, the calcium channels
close, while the potassium channels continue to conduct potassium out of the cell; in this way, the electronegative membrane potential is restored.7 One of the potassium currents (Ikr), located on the myocyte cell membrane, is mostly responsible for the potassium efflux seen during phases 2 and 3 of the cardiac action potential.10 For reasons that are not well understood, these Ikr currents are sensitive to extracellular potassium levels, and as the potassium levels increase in the extracellular space, potassium conductance through these currents is increased so that more potassium leaves the myocyte in any given time period.10 This leads to an increase in the slope of phases 2 and 3 of the action potential in patients with hyperkalemia and therefore, to a shortening of the repolarization time. This is thought to be the mechanism responsible for some of the early electrocardiographic manifestations of hyperkalemia, such as ST-T segment depression, peaked T waves, and Q-T interval shortening.

As illustrated in
Figure 4, Vmax is greatest when the resting membrane
potential at the onset of the action potential is approximately
–75 mV, and does not increase as the membrane
potential becomes more negative. Conversely,
as the resting membrane potential becomes less negative
(that is, –70 mV), as in the setting of hyperkalemia
(Fig. 3), the percentage of available sodium
channels decreases. This decrease leads to a decrement
in the inward sodium current and a concurrent
decrease in the Vmax; therefore, as the resting membrane
potential becomes less negative in hyperkalemia,
Vmax decreases. This decrease in Vmax causes a slowing
of impulse conduction through the myocardium
and a prolongation of membrane depolarization; as a
result, the QRS duration is prolonged.
Hypokalemia would hyperpolarize the resting membrane potential but this does not change the slope of phase 0 as the Vmax does not change (Fig. 4).
Causes of Hyperkalemia
Numerous causes of hyperkalemia are seen in clinical
practice. The most common are renal disease and the
ingestion of medications that predispose the patient
to hyperkalemia.2 Medications known to cause hyperkalemia
include angiotensin-converting enzyme inhibitors,
angiotensin-receptor blockers, penicillin G,
trimethoprim, spironolactone, succinylcholine, alternative medicines, and heparin.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1413606/pdf/20060300s00010p40.pdf
4. Describe how surreptitious use of diuretics can cause hypokalemia and explain how one diuretic (acetazolamine) can be used to treat hypokalemia.
CA inhibitors, like acetylzolamide, are effective in many cases of Hypokalemic periodic paralysis. This is at first a paradox because CA inhibitors cause potassium loss and hypokalemia. However, CA inhibitors also impair bicarbonate reabsorption in the renal tubules. The resulting urinary loss of bicarb causes metabolic acidosis. The increased hydrogen ion causes a shift of potassium out of cells, alleviating the hypokalemia. Also results in less Ca++ binding to Protein-, increasing contractability.
5. Explain the mechanisms of muscle weakness in hypokalemia.
Low potassium causes vasoconstriction and reduced muscle blood flow, leading to lactic acid accumulation in muscles. This causes osmotic entry of water which impairs calcium channels. Reduced calcium movement impairs contraction.
Hypokalemia will decrease potassium channel conductance, which will lengthen repolarization time of a nerve cell. If this gets to be severe enough, transmission of action potentials will be disrupted, and the result can be generalized weakness or paralysis because signaling to the muscles are disrupted.
Hyperkalemia also causes muscle weakness:
It might be expected that this depolarization would make it easier to generate action potentials in the muscle because the resting membrane potential would be closer to threshold. A more important effect of depolarization, however, is that it closes the inactivation gates on Na + channels. When these inactivation gates are closed, no action potentials can be generated, even if the activation gates are open. Without action potentials in the muscle, there can be no contraction.
6. Describe the genetics and molecular mechanisms of hypokalemic periodic paralysis.
The physiologic basis of flaccid weakness is inexcitability of the muscle membrane (ie, sarcolemma). Alteration of serum potassium level is not the principal defect in primary PP; the altered potassium metabolism is a result of the PP. In primary and thyrotoxic PP, flaccid paralysis occurs with relatively small changes in the serum potassium level, whereas in secondary PP, serum potassium levels are markedly abnormal.
The sodium channel has 2 gates (activation and inactivation) and can exist in 3 states. At rest with the membrane polarized, the activation gate is closed and the inactivation gate is opened. With depolarization, the activation gate opens, allowing sodium ions to pass through the ion channel and also exposing a docking site for the inactivation gate. With continued depolarization, the inactivation gate closes, blocking the entry of sodium into the cell and causing the channel to enter the fast-inactivation state. This inactivation of the channel allows the membrane to become repolarized, resulting in a return to the resting state with the activation gate closed and the inactivation gate opened. Two inactivation processes occur in mammalian skeletal muscle: Fast inactivation involves terminating the action potential and acts on a millisecond time scale. Slow inactivation takes seconds to minutes and can regulate the population of excitable sodium channels.
Sodium channel mutations that disrupt fast and slow inactivation are usually associated with a phenotype of HyperPP and myotonia, where as mutations that enhance slow or fast inactivation producing loss of sodium channel function cause HypoPP.
some forms of HypoPP involve mutations of calcium and/or potassium channels.
7. Explain the mechanisms that lead to transcellular shifts of potassium. Describe how marijuana intoxication may lead to hypokalemia.
Electrolyte abnormalities reported in marijuana users contribute to pathology. Chronic marijuana users have lower serum sodium and potassium than non-users.[17] The heavy consumption of carbohydrates while intoxicated leads to an increase in serum insulin levels, driving potassium into cells and causing serum hypokalemia.[18]
The heavy consumption of carbohydrates while intoxicated leads to an increase in serum insulin levels, driving potassium into cells and causing serum hypokalemia.[18] This hypokalemia can produce reentrant arrhythmias by decreasing conductivity and increasing the resting membrane potential, duration of the action potential, and duration of the refractory period.[19] EKG changes include the decrease in T-wave amplitude, presence of U waves and a prolonged QTc.
Memory tool: Al Klow sis
8. Bonus question (anybody can do this one): Explain the abnormal findings on the EKG.
This hypokalemia can produce reentrant arrhythmias by decreasing conductivity and increasing the resting membrane potential, duration of the action potential, and duration of the refractory period.[19] EKG changes include the decrease in T-wave amplitude, presence of U waves and a prolonged QTc.

The decrease in Vmax in hyperkalemia causes a slowing of myocardial
conduction, manifested by progressive prolongation of the P wave, PR interval, and QRS complex.
The maximum conductance of these channels occurs approximately 50 msec after the initiation of phase 0 and is reflected in phase 2 of the action potential.
During phase 2, potassium efflux and calcium influx offset one another so that the electrical charge across the cell membrane remains the same, and the so-called plateau phase of the action potential is created (Fig. 3). During phase 3, the calcium channels
close, while the potassium channels continue to conduct potassium out of the cell; in this way, the electronegative membrane potential is restored.7 One of the potassium currents (Ikr), located on the myocyte cell membrane, is mostly responsible for the potassium efflux seen during phases 2 and 3 of the cardiac action potential.10 For reasons that are not well understood, these Ikr currents are sensitive to extracellular potassium levels, and as the potassium levels increase in the extracellular space, potassium conductance through these currents is increased so that more potassium leaves the myocyte in any given time period.10 This leads to an increase in the slope of phases 2 and 3 of the action potential in patients with hyperkalemia and therefore, to a shortening of the repolarization time. This is thought to be the mechanism responsible for some of the early electrocardiographic manifestations of hyperkalemia, such as ST-T segment depression, peaked T waves, and Q-T interval shortening.