Khan video on diffusion
This is a good video but does not mentioned the influence of capillary volume and hemoglobin.
Capillary volume is part of the surface area component (alveolar surface area + capillary volume) of the Fick Equation and is influenced by factors such as exercise which increases diffusing capacity by increasing blood flow to the top of the lungs and thereby increasing capillary volume = surface area for diffusion. The Fick equation may be simplified by combining (A x K)/T into a single parameter, DL, the diffusing capacity of the lung.
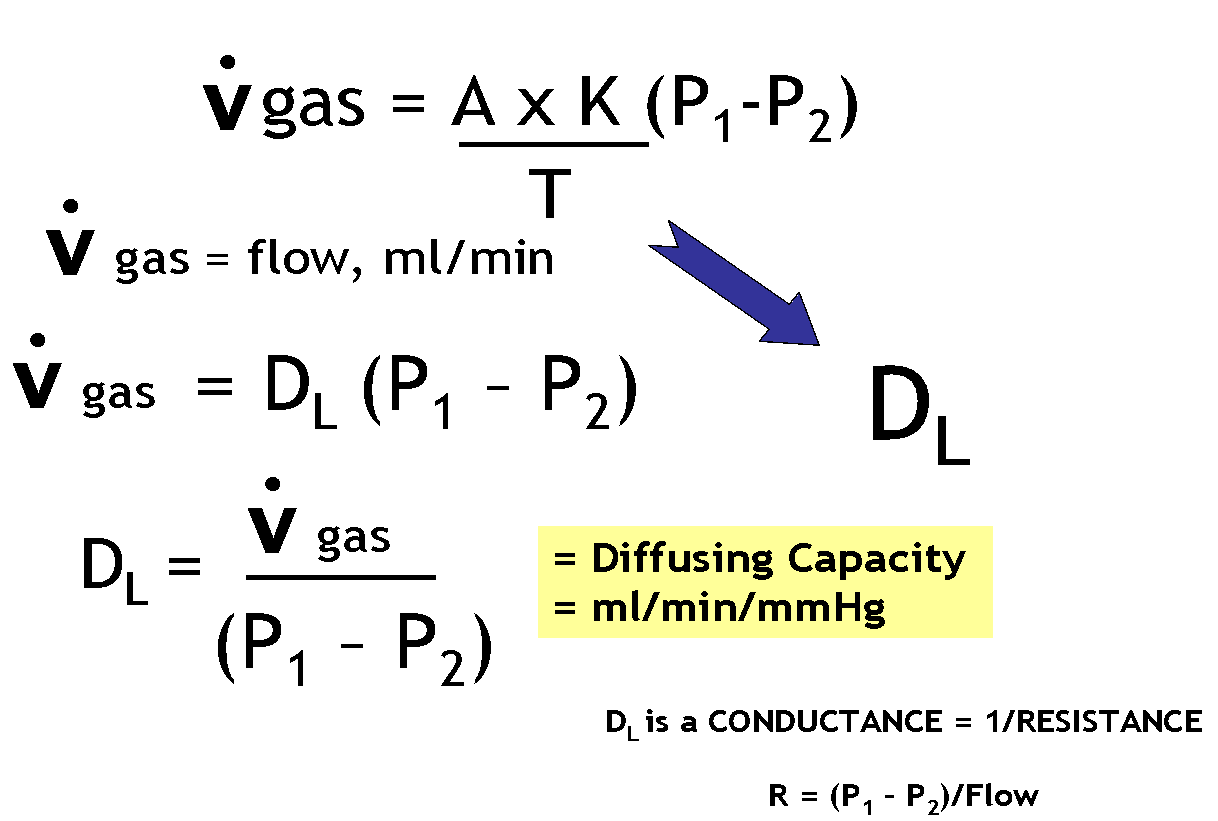
Passive diffusion proceeds at a rate proportional to the driving force (P1 – P2), surface area (A), and solubility of the diffusing gas (K) and inversely proportional to thickness of the barrier (T). These factors comprise Fick’s law for passive diffusion, where K is Krogh’s diffusion constant. Because it is not possible to accurately measure area or thickness, these membrane properties along with K are lumped to form a parameter called diffusing capacity, DL. As shown in the figure, the flow of gas by diffusion, in ml/min, = DL (P1 – P2). Note that when P1 = P2, the driving pressure becomes zero and gas movement stops. This equation for gas flow can be rearranged to provide the equation for diffusing capacity: DL = Vgas / (P1 – P2)
Hemoglobin concentration is important in the rate of diffusion because the final step in diffusion of oxygen is reaction with hemoglobin. In fact, the reaction rate of with hemoglobin accounts for about half of the total resistance to oxygen uptake in the lungs. This means that anemia can result in impaired diffusion.
Also, as described below, diffusing capacity is measured using carbon monoxide. The binding of CO to Hb goes faster with more Hb; e.g., anemia will reduced the measured diffusing capacity.
Also, as described below, diffusing capacity is measured using carbon monoxide. The binding of CO to Hb goes faster with more Hb; e.g., anemia will reduced the measured diffusing capacity.
How is Diffusing Capacity Measured?
Carbon monoxide is used to measure diffusing capacity of the lung (DL). Advantages of CO are that its uptake is limited by membrane properties (diffusion limited) and not by blood flow (perfusion limited). This is so because CO gas binds 100% with hemoglobin meaning there is no back pressure (P2) to slow or stop diffusion. Since P1 is kept constant, the rate of transfer depends only on DL. 
https://www.openanesthesia.org/pulm-diffusing-capacity/
Pulmonary diffusing capacity is often measured by Diffusion capacity of the Lungs for carbon monoxide (DLCO). In essence, this measures how much CO can pass from the alveoli to the blood in the pulmonary capillaries, thus giving clinicians the broader idea of how much inhaled gas can pass into the blood through the lungs.
While some state the “DLCO correlates with the total functioning surface area of the alveolar-capillary interface (Butterworth, et al),” Dr. McCormack notes, “Older textbooks suggest that thickening of the alveolar-capillary membrane (in interstitial lung disease) and loss of alveolar membrane surface area (in emphysema) are the primary causes of a low DLCO. However, subsequent experimental data suggest these and most other diseases that influence the DLCO do so by reducing the volume of red blood cells in the pulmonary capillaries” (McCormack). Regardless of theory, whether the surface area or the alveolar surface itself is modified or the volume of the blood in the pulmonary capillaries is modified, the DLCO reflects how much gas can be transferred to the blood via the lungs.
- Butterworth IV, JF, Mackey DC, Wasnick JD. Morgan & Mikhail’s Clinical Anesthesiology, 5th ed. New York, NY: McGraw Hill; 2013.
- McCormack, Meredith. “Diffusing Capacity for Carbon Monoxide.” Ed. James Stoller and Helen Hollingsworth. N.p., 14 Apr. 2015. Web.

